Psychiatry damages your brain
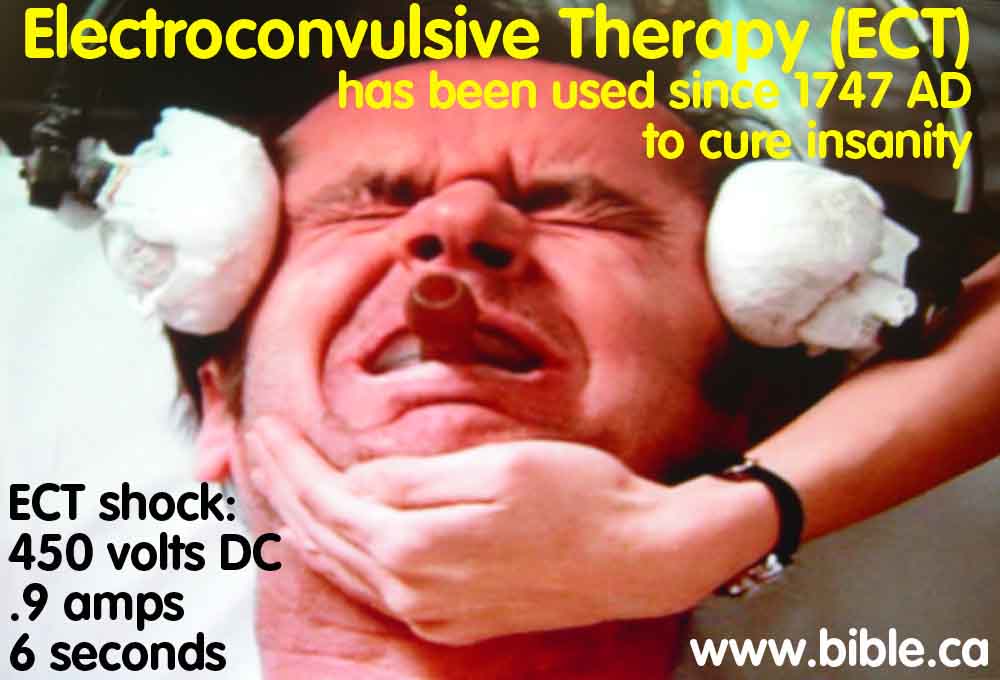
Electroconvulsive Therapy
(ECT).9 amps at 450 volts DC for 6 seconds
(enough to an 84 watt light bulb)
Electroconvulsive Therapy
(ECT).9 amps at 450 volts DC for 6 seconds
(enough to an 84 watt light bulb)
Summary:
In 1938, Ugo Cerletti conceived Electroconvulsive Therapy (ECT), while he observed how pigs at a slaughter house were shocked into unconsciousness, then killed by slitting the throat. He noted that it was not the shock did not actually killed the pigs. Being a specialist in epilepsy, this is where Cerletti first got the idea of shocking the human brain to cure schizophrenia and the invention of ECT. Using electricity to cure insanity has a long history dating back to Charles Wesley, the founder of Methodism in 1747 AD. With ECT people undergo 5 - 20 shocks over several weeks. The shock is enormous and uses 450 volts DC in pulsed square waves at a current of .9 Amps for 6 seconds. ECT is a form of electric lobotomy. A single ECT treatment passes enough electricity through your brain to light an 84 watt light bulb for 6 seconds or a 500 watt halogen light for 1 second. ECT has been documented to cause death, strokes and tissue damage. "PA-PSRS has received five reports of patients experiencing skin burns or injuries from a fire during electroconvulsive therapy (ECT) treatments. ... in the report of a fire, a bright flash and flames were noted on the right side of the patient's head at the instant that the ECT shock was given. Though the flames were quickly extinguished, the patient experienced first and second-degree burns on one ear and first-degree burns on the forehead above one eye." (Skin Burns and Fires during Electroconvulsive Therapy Treatments, PA-PSRS Pennsylvania Patient Safety Advisory, Vol. 4, No. 1, March 2007) The original theories for ECT treatment were founded on the invalid idea that epileptics were never schizophrenic and that the two conditions were mutually exclusive and could not co-exist. Therefore it was originally thought that inducing epileptic convulsions would cure schizophrenic. Although we know today that this is just another example of psychiatric quackery theory, ECT effectively disables brain function by wiping out memories that make us sad and cause depression. Entire university educations were erased from people's minds. "Memory Loss: ECT is a common cause of severe retrograde amnesia, i.e.. destruction of memories of events prior to an injury. The potency of ECT as an amnestic exceeds that of severe closed head injury with coma. It is surpassed only by prolonged deficiency of thiamine pyrophosphate. bilateral temporal lobectomy, and the accelerated dementias, such as Alzheimer's. After ECT it takes 5 to 10 minutes just to remember who you are. where you are. and what day it is." (Shock Treatment, Brain Damage, and Memory Loss: A Neurological Perspective, John M. Friedberg, Neurosurgeon, American Journal of Psychiatry 134:9, September 1977. p 1010-1013) ECT has been outlawed in many countries and will likely experience a global ban by 2015 AD. New quackery treatments that shock the brain, include Deep brain stimulation, which surgically embeds an two "meat thermometer looking" electrodes 6 inches in the middle of your brain to apply shocks. Vagus Nerve Stimulation wraps an electrode around the vagus nerve in your neck and applies shocks through a surgically embedded "pacemaker of the nerve". Passive brain shocking systems include Repetitive Transcranial Magnetic Stimulation, which uses magnetic induction to shock the brain in an area the size of a quarter, about 2 inches below the skull. Shocking the brain with electricity interferes with the normal electric function of the brain, which normally runs on a voltage of 1/10th of a single volt. ECT applies up to 450 volts, which is about 4500 times higher voltage than what the brain uses. ECT to the brain, is like hooking your 120 volt big screen TV up to 540,000 volts and expecting an improved picture! For more details, read our other book called, "Everything I ever needed to know about how ECT causes brain and tissue damage, I learned in my grade 9 introductory electricity shop class." (Electroconvulsive Therapy, ECT)
Introduction:
- ECT is one of the strangest ideas that chemical psychiatrists have invented to cure people of insanity. On one hand these psychiatrists believe that depression is caused by chemical imbalances of the brain or bad brain wiring, on the other they use ECT to wipe out memories that are causing the depression. This stunning cognitive dissonance between etiology and treatment is something only a psychiatrist could rationalize. On one hand they blame depression on brain chemicals, on the other, they treat by wiping out memories by shocking the brain. Church ministers, for example agree that depression is caused by dwelling on bad stuff that has happened to them but reject shocks to remove the memories, or drugs that make one indifferent to bad memories.
- ECT today, uses 450 volts DC in pulsed square waves at a current of .9 Amps for 6 seconds. People undergo 5 - 20 shocks over several weeks. Today they are put under anesthesia so they do not feel a thing.
- Studies have proven that ECT works no better than a placebo. People were told they were shocked when they came to, when they were not, However they were "cured" as if they had been shocked. These stories and studies are numerous.
- "ECT stands practically alone among the medical/surgical interventions in that misuse was not the goal of curing but of controlling the patients for the benefits of the hospital staff" (David J. Rothman, Medical Historian, NIH Consensus Conference on ECT, 1985 AD)
- "From a neurological point of view ECT is a method of producing amnesia by selectively damaging the temporal lobes and the structures within them. When it was first introduced it was only one of several methods of producing brain damage employed in psychiatry, including insulin coma (1927) camphor and Pentylenetetrazol (Metrazol) injections (1933). and prefrontal lobotomy (1935), it is the only such method from that era still used on a large scale. It is highly unlikely that ECT, if critically examined, would be found acceptable by today's standards of safety. From a neurological point of view ECT produces form of brain disease. with an estimated incidence new cases in the range of 100.000 per year. Many psychiatrists are unaware that ECT causes brain damage and memory loss because numerous authorities and a leading psychiatric textbook deny these facts. Others, who know of its effects argue that the interruption of unpleasant states of mind is worth the damage. Some are beginning to give the client a truly informed choice, although state laws still allow ECT to be imposed if the doctor feels that ''good cause'' exists. Assuming free and fully informed Consent, it is well to reaffirm the individual's right to pursue happiness through brain damage if he or she so chooses. But we might ask ourselves whether we, as doctors sworn to the Hippocratic Oath, should be offering it." (G. Shock Treatment, Brain Damage, and Memory Loss: A Neurological Perspective, John M. Friedberg, American Journal of Psychiatry 134:9, September 1977)
- Psychiatry has a long history of hurting, torturing and injuring people.
- We predict that by 2015, ECT will be outlawed because of the dramatic increase in civil litigation from the brain damage people suffer at the hands of chemical psychiatrists.
- For hundreds of years people were put on a starvation diet, given drugs to make them nauseous for weeks on end and water tortured.
- "It appears that neither psychiatrists, nor the editors of medical and scientific publications, nor the media, nor the public feel the need to reconcile the contradiction of treating the same brain disease with interventions as different as ECT, VNS, DBS, TMS, antidepressant drugs, cognitive therapy, various "talk therapies," and dolphin therapy. At this point, it may be well to recall that the so-called effectiveness of this kind of therapeutic hocus-pocus had been investigated more than two hundred years ago by some of the greatest scientific figures of the time who had no difficulty concluding that the miracle-cure they were examining—Mesmerism—was simply bogus. Just as importantly, they also concluded that because healer and healed are equally deceived and self-deceived, the effectiveness of the hocus-pocus therapy appears real, at least for a while. Then, after they are debunked, they lose their effectiveness and are soon replaced by new miracle cures. Mesmer first used magnets to cure patients. Then his mere touch turned out to be curative. Finally, he didn't even have to touch patients to cure them—they could cure themselves and each other by means of rituals that utilized the powers of an imaginary magnetic fluid, a property of "animal magnetism." Between 1774 and 1777, in a mere three years, Mesmer rose from obscure physician to world-famous healer, only to be exposed as a quack." (Coercion as Cure, Thomas Szasz, 2007 AD, p 148)
- In the early 1900's psychiatrists invented the lobotomy which shoved a blunt knife through the eye sockets into the brain to cut nerves connecting the two frontal lobes of the brain.
- Electric shock therapy was invented by Charles Wesley, the founder of Methodism in 1747 AD. The amount of electricity Wesley used was more like a static shock you would experience from rubbing your feet on the carpet.
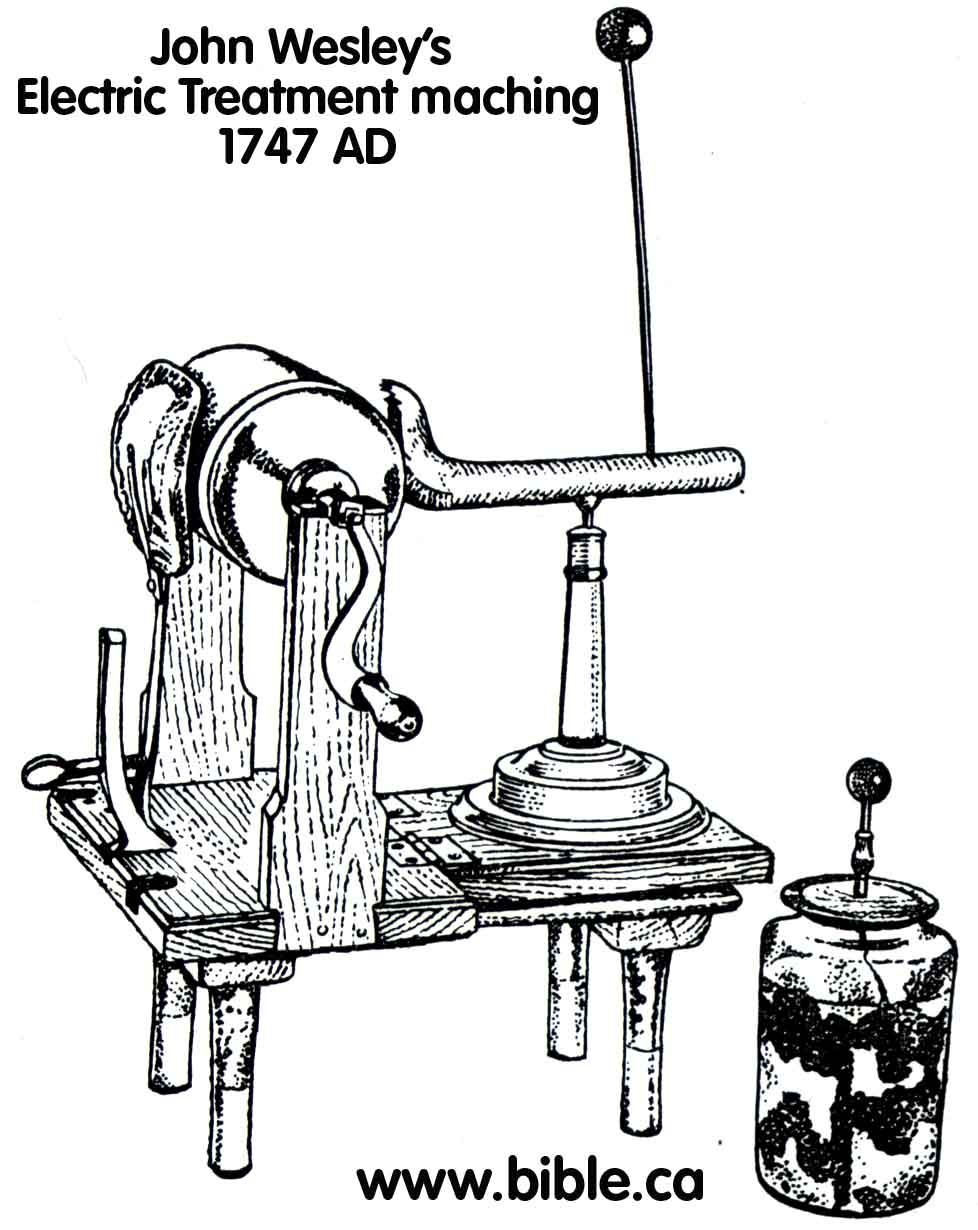
- It wasn't till about the 1938 that they started shocking the brain with huge amounts of electricity.
- A single ECT treatment passes enough electricity through your brain to light an 84 watt light bulb for 6 seconds or a 500 watt halogen light for 1 second. And we call this medicine?
A. ECT Flames causing 1st degree burns in 2007:
- The amount of electricity used in ECT is huge. It is not surprising that fires happen.
- What this report proves, is what every electrician understands. The fire is caused by a gap that allowing the current to ark between the electrode and the skin. It is exactly like giving someone a static shock after rubbing your feet on the carpet. ECT technicians must ensure that there is direct contact between the electrode and the skull. Any gap will cause a fire and burn the patient.
- While this is rare, it demonstrates the huge amounts of electricity that is passed through the brain.
- "PA-PSRS has received five reports of patients experiencing skin burns or injuries from a fire during electroconvulsive therapy (ECT) treatments. The first report described sparks but no fire; the anesthesiologist and RN observed this event at the time of the ECT device activation. The patient experienced erythematous skin on one side of the forehead and behind one ear. The second report described burns to the patient's hair and skin in the temporal area in front of one ear. In the third skin burn report, a post-anesthesia care unit nurse noted burn-like lesions on the patient's earlobe and forehead; however, according to the report, clinical staff believed the lesions were pre-existing to the ECT treatment. In the fourth report, a flash was noted at the electrode sites on both sides of the patient's temples. The flash occurred at the time a staff member turned the device off then on again because the display screen was blank (i.e., no illumination). According to the facility, although an oxygen (O2) face mask was applied to the patient, no O2 was flowing at the time of the flash. Finally, in the report of a fire, a bright flash and flames were noted on the right side of the patient's head at the instant that the ECT shock was given. Though the flames were quickly extinguished, the patient experienced first and second-degree burns on one ear and first-degree burns on the forehead above one eye. ... Electrode Site Preparation: Under the right conditions, skin burns during ECT treatment may occur readily due to poor electrode contact with the skin. Electrode site preparation is an important step in ensuring adequate electrode-to-skin contact. Hair, dead skin, and even cosmetic products between the electrode and skin could result in poor contact." (Skin Burns and Fires during Electroconvulsive Therapy Treatments, PA-PSRS Pennsylvania Patient Safety Advisory, Vol. 4, No. 1, March 2007)
B. The shocking facts about ECT:
- "In ECT, 180 to 460 volts of electricity are fired through the brain, for a tenth of a second to six seconds, either from temple to temple (bilateral ECT) or from front to back of one side of the head (unilateral ECT)." (The Hidden Side of Psychiatry: Electroconvulsive Therapy, Gary Null, Ph.D., 1999)
- "Electroconvulsive therapy (ECT) has been proven quite effective and is used mainly for chronically depressed people who have not responded to drug therapy. In 1938, when ECT was first introduced, wide-awake patients were strapped to a table to prevent them from hurting themselves during the convulsions, and were shocked (jolted) with 100 volts of electricity to the brain." (Study Guide, Therapy, Richard O. Straub, 1995, Ch 16, p 414)
- "ECT parameters were conventional. i.e. 130 volts for 0.3 seconds." (Shock Treatment, Brain Damage and Memory Loss: A Neurological Perspective. John M. Friedbarg, American Journal of Psychiatry. September 1977, 134: 9, p 1010-1013)
- "In the meantime, however, with the assistance of a technician, [Lucio] Bini had constructed a primitive apparatus that would permit application of 80 to 100 volts of electricity for a fraction of a second." (Alternatives: Electroshock, A History of Psychiatry, Edward Shorter, 1997, p 218)
- "The preferred and now standard mode of achieving seizure was introduced by the Italian physicians Ugo Cerletti and Lucio Bini in 1938. Their standard technique, the basics which remain in use today, was to apply, via electrodes placed in the temporal region of both sides of the head, 'wall socket' alternating current (AC) between 70 to 150 volts for 0.1 to 1.0 seconds." (Electroconvulsive therapy. Encyclopedia of Psychology, Robert C. Carson, Vol 3. 2000, p 155-156)
- "It was also known in this early period that voltage applied to the head, as in legal electrocution, produced hemorrhage and rupture of cranial contents. Ugo Cerletti demonstrated that the electricity in the range of 100 V and 200 mA is rarely fatal when current path is confined to the head." (Shock Treatment, Brain Damage, and Memory Loss: A Neurological Perspective, John M. Friedberg, American Journal of Psychiatry.134, 9, September 1977, p 1010)
- "One does not need a medical degree to recognize the destructive potential of passing 100 to 150 volts of electricity through the human brain." (Electroshock: Death, Brain Damage, Memory Loss and Brainwashing, Slife, Brent, 1994, p 291)
C. The electric shock output of ECT machines:
- The laws of electricity:
Voltage (V) = Current (I) x Resistance (R)
Charge (Q) = Voltage (V) x Current (I) x Time (T) = V x I x T
T = (2 x Frequency of pulses) x pulse time (t) x Treatment time (tt)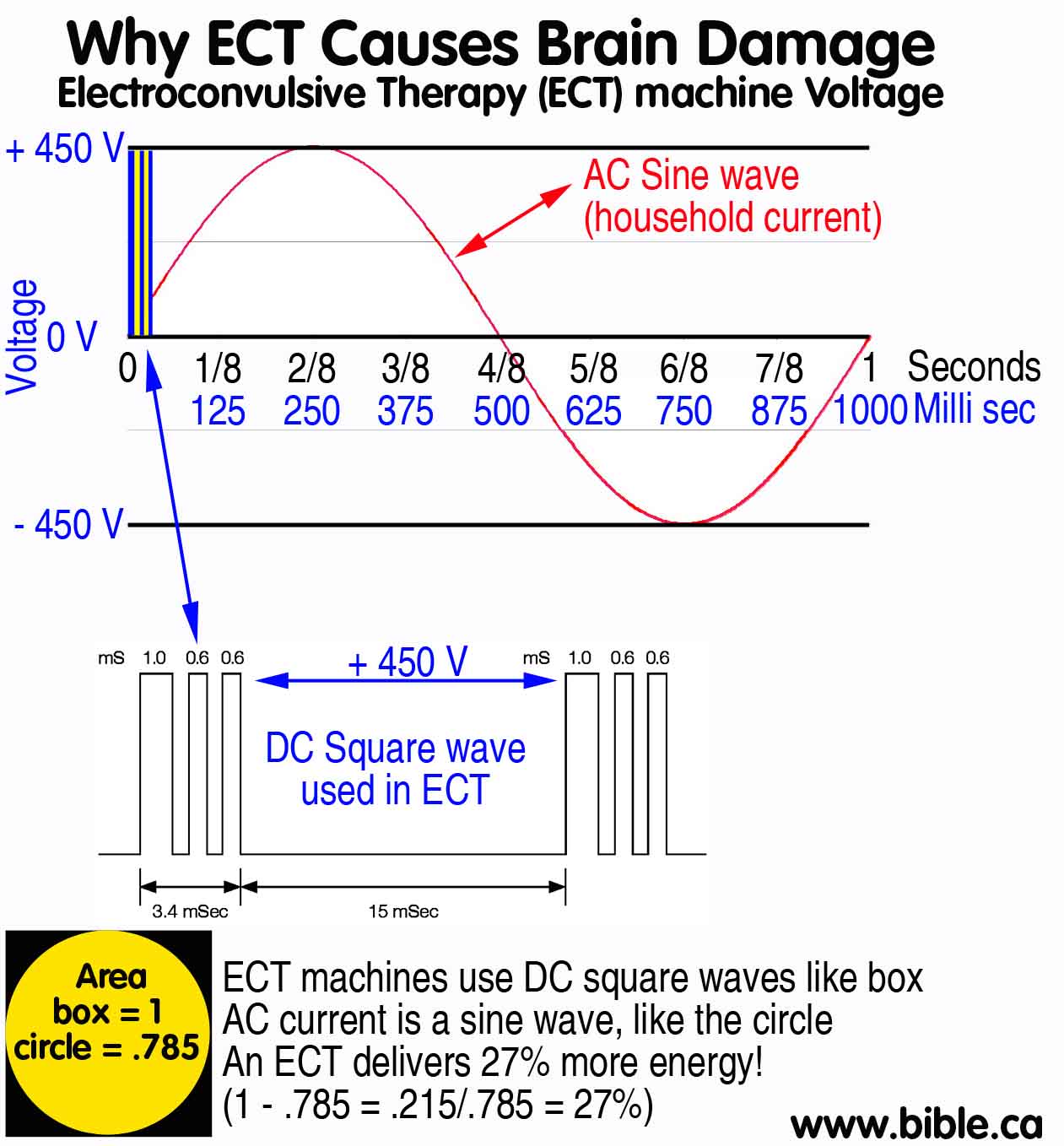
- All ECT machines put out a fixed current (I) of about .9 amps. (9/10ths of one amp or 90 milliamps) Because each human skull has a different resistance, the voltage is variable. If you stuck a probe from an ohm meter through the skin into the skull cap, all humans would measure at about the same resistance. Since ECT machines do not penetrate the skin, the resistance varies primarily because of surface moisture. For example, some electricians with dry hands, actually touch household current wires to see if they are live or not. But if he did it with wet hands, he would get a "larger shock" in that the voltage is still 120 v, but the current is much higher because the water reduced the resistance. This is how the V=IxR formula works. Since the resistance between the temples varies because of how moist that person's skin is, the voltage must be variable in order to achieve a constant current (I) of .9 amps.
- Now household alternating current is a standard sine wave. But ECT use pulsed square waves. The frequency (F) is 70 ht and the duration is 1.5 ms. Since there are two pulses of 1.5 ms for each cycle (F), that means there are 140 pulses of 1.5 ms every second at .9 amps. This is equal to a continuous pulse of 210 ms (1/5th second), ever second. To quantify this differently, you touch a live wire for 1/5th of a second. If you were experience the shock of an ECT machine, you would touch a live wire at 450 volts for 1/5th of a second, for 6 seconds. The total shock from a six second zap of an ECT machine would be like getting continuously shocked at 450 volts for over a second. That's a huge shock!
- But it gets worse. Standard alternating current sine waves at 450 volts AC deliver much less energy than DC pulsed square waves. For example a simple way to quantify the difference in energy between a sine and square wave, is to compare the volume of a square and a circle of the same width. This is simple to calculate. a 1 inch box has an area of 1 square inch. A 1 inch circle has an area of piR2 = 3.14 x .5 x .5 = .785
- When a machine is rated at 70 ht, this means that it delivers 140 square wave pulses of electricity every second. This is the same as AC current except instead of a positive pulse (+ve) and a negative pulse (-ve) every second, the machine rectifies the sine wave and creates two positive square waves each cycle.
- The formula to calculate the Time (T) to be used in ohms law is as follows: Frequency (F) x pulse time (t) x Treatment time = F x tt x t.
- Since all ECT machines have a "rated frequency" of 70 Hz, this means the actual frequency is 140 ht.
- A sine wave voltage fluctuates between zero and 450 volts twice a second but DC current is continuously 450 volts. Thus DC current puts out 27% more Charge (Q) than AC current. This can be calculated by comparing the areas of a 1 inch box and a 1 inch circle. A 1 inch circle has an area of piR2 = 3.14 x .5 x .5 = .785. To calculate the percentage difference in Charge (Q) we take the area of the circle, subtract the area of the square and calculate the ratio: 1 - .785 = .215/.785 = 27%.
- So when we want to equate the amount of current passing through the brain in terms of household current, we must use the following formula: Square wave Charge = 1.27 (Q) x Sine wave Charge (Q)
Machine
|
Current (I)
V/R Fixed |
Voltage (V)
IxR Variable |
Rated
Frequency |
Square wave Pulses/s
(F) |
Treatment Time
(tt) |
Pulse
(t) |
Time
(T) Fxttxt |
Charge (Q)
IxT milli coulombs |
Thymatron
|
0.9 Amps
|
450 Volts
|
70 Ht
|
140Ht
|
1-6 s
|
1.5ms
|
1.25s
|
504 mC
|
Ectron
|
0.75 Amps
|
225 Volts
|
70 Ht
|
140Ht
|
1-12 s
|
1.5ms
|
2.5s
|
1000 mC
|
Mecta
|
0.8 Amps
|
240 Volts
|
70 Ht
|
140Ht
|
1-6 s
|
1.5ms
|
1.25s
|
576 mC
|
D. Thymatron System IV (Manufacturers Specifications)
- Stimulus Output: Current: 0.9 amp constant, limited to 450 volts
- Frequency: 10 to 70 Hz in 10 Hz increments (to 140 Hz for 0.25 ms pulse).
- Pulsewidth: 0.25 to 1.5 msec in 0.25 msec increments.
- Duration: 0.14 to 8.0 sec in increments of equal charge.
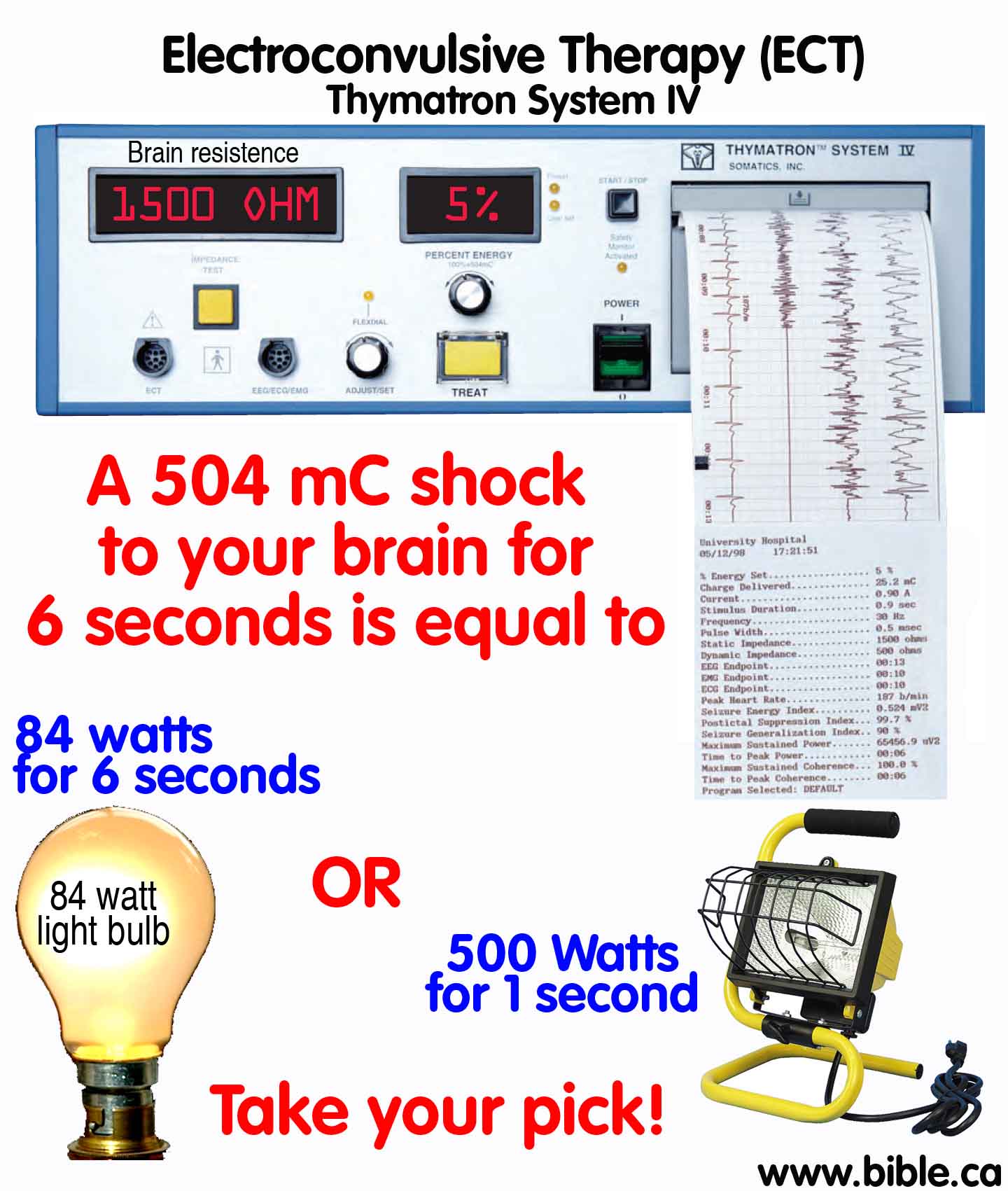
- Maximum output: Standard maximum output across 220 ohms impedance: 504 milliCoulombs, 99.4 joules.
- Output with double-dose option (where available) across 220 ohms impedance: 1008 mC, 198.8 joules
E. Comparing and ECT to light bulbs:
- We know that the most popular ECT used in the USA (Thymatron) delivers 504 millicoulombs of shock charge to the brain. How many standard 60 watt light bulbs does this equal?
- Charge (Q) = Voltage (V) x Current (I) x Time (T) = V x I x T
- Charge (504) = Voltage (120) x Current (?) x Time (6)
- current = charge (504)/ Voltage (120) x Time (6) = 504 divided by (120x6) = 504/720 = .7 Amps
- Watts = VA = 120 x .7 = 84 watts for 6 continuous second.
- So getting a single ECT treatment is equivalent to putting enough power through your brain to light an 84 watt light bulb for six continuous second.
- If this shock was only 1 second long, it would be enough power to light six 84 watt light bulbs or a single 504 watt light bulb.
- Take your pick! Your brain can light up an 84 watt light bulb for 6 seconds or a 504 watt light bulb for 1 second.
F. The Father of ECT: Ugo Cerletti
"Convulsions were to be induced with a therapeutic aim since the good clinical results obtained by Meduna's method were ascribed to them. For this the old transcranial method followed by physiologists was sufficient. But this idea then, and for a long time to come, appeared Utopian, because of the terror with which the notion of subjecting a man to high-tension currents was regarded. The spectre of the electric chair was in the minds of all and an imposing mass of medical literature enumerated the casualties, often fatal, ensuing upon electric discharges across the human body. Nowadays, after twelve years of experience with electroshock, that terror may seem to have been exaggerated; but cases of death caused by low tensions (forty volts) had been described. Since, to obtain fits in dogs, tensions of around 125 volts were used, moreover with an alternating current which was held to be more dangerous than direct - it seemed evident that these experiments were too near the danger zone to have any possibility of being applied to man. The fact is that no one at the clinic seriously thought of applying electric convulsions to man, even though experiments continued upon dogs, both with electricity and with Cardiazol. So, over a year went by. Nevertheless I, who had gone to such lengths in striving to preserve dogs from death when given electrically induced convulsions, had now come to the conviction that a discharge of electricity must prove equally harmless to a man if the duration of the current's passage were reduced to a minimum interval. Continually turning the problem over in my mind I felt that I would sooner or later be able to solve it; so much so that in 1937, not being able to go to the Munsingen Congress, I allowed Bini to hint at these vague hopes, and I, myself, at the 1937 Milan Assembly concerning the therapeutics of schizophrenia, announced these hopes that I had been nourishing. This inactivity in the face of so momentous a question greatly depressed me, so that I immediately jumped at the information, given me by my colleague, Professor Vanni, that 'at the Rome slaughterhouse pigs are killed by electricity'. As though to justify my passiveness and to settle my hopes by facing a real fact, I decided to see this electric slaughtering with my own eyes, and immediately went to the slaughterhouse . There I was told that the application of a current across the pigs' heads had been in use for some years. The butchers took hold of the pigs near their ears with a large scissor-shaped pair of pincers. The pincers were connected to the lighting plant with wires, and terminated in two teethed disc-electrodes enclosing a sponge wet with water. As they were seized, the pigs fell on their sides and were soon taken by fits (convulsed). Then the butcher, taking advantage of the unconscious state of the animal, gave its neck a deep slash, thus bleeding it to death. I at once saw that the fits were the same as those I had been producing in dogs, and that these pigs were not being 'killed by electricity', but were bled to death during the epileptic coma. Since a great number of pigs was available at the slaughterhouse for killing, I now set myself the exact opposite of my former experiments' aims; namely, no longer to make efforts to keep the convulsed animals alive, but rather to determine what the conditions must be for obtaining their death by an electric current. Having obtained authorization for experimenting from the director of the slaughterhouse, Professor Torti, I carried out tests, not only subjecting the pigs to the current for ever-increasing periods of time, but also applying the current in various ways: across the head, across the neck, and across the chest. Various durations (twenty, thirty, sixty or more seconds) were tried. It turned out that the more serious results (prolonged apnea sometimes lasting many minutes and, exceptionally, death) appeared when the current crossed the chest; that this application was not mortal for durations of some tenths of a second; and, finally, that passage of the current across the head, even for long durations, did not have serious consequences. It was found that pigs, even when treated in this last way several times, 'came to' gradually, after a fairly long interval (five to six minutes), then started moving, next made various attempts to get shakily to their feet, and finally ran rapidly to mix with their mates in the pen. These clear proofs, certain and oft repeated, caused all my doubts to vanish, and without more ado I gave instructions in the clinic to undertake, next day, the experiment upon man. Very likely, except for this fortuitous and fortunate circumstance of pigs' pseudo-electrical butchery, electroshock would not yet have been born. A schizophrenic of about forty, whose condition was organically sound, was chosen for the first test. He expressed himself exclusively in an incomprehensible gibberish made up of odd neologisms, and since his arrival from Milan by train without a ticket, not a thing had been ascertainable about his identity. Preparations for the experiment were carried out in an atmosphere of fearful silence bordering on disapproval in the presence of various assistants belonging to the clinic and some outside doctors. As was our custom with dogs, Bini and I fixed the two electrodes, well wetted in salt solution, by an elastic band to the patient's temples. As a precaution, for our first test, we used a reduced tension (seventy volts) with a duration of 0 2 second. Upon closing the circuit, there was a sudden jump of the patient on his bed with a very short tensing of all his muscles; then he immediately collapsed onto the bed without loss of consciousness. The patient presently started to sing at the top of his voice, then fell silent. It was evident from our long experience with dogs that the voltage had been held too low. I, bearing in mind the observations with repeated applications of the day before upon pigs, made arrangements for a repetition of the test. Someone got nervous and suggested whisperingly that the subject be allowed to rest; others advised a new application to be put off to the morrow. Our patient sat quietly in bed, looking about him. Then, of a sudden, hearing the low toned conversation around him, he exclaimed - no longer in his incomprehensible jargon, but in so many clear words and in a solemn tone - 'Not a second. Deadly! ' The situation was such, weighted as it was with responsibility, that this warning, explicit and unequivocal, shook the persons present to the extent that some began to insist upon suspension of the proceedings, Anxiety lest something that amounted to superstition should interfere with my decision urged me on to action. I had the electrodes reapplied, and a 110-volt discharge was sent through for 0.5 second. The immediate, very brief cramping of all the muscles was again seen; after a slight pause, the most typical epileptic fit began to take place. True it is that all had their hearts in their mouths and were truly oppressed during the tonic phase with apnea, ashy paleness, and cadaverous facial cyanosis - an apnea which, if it be awe-inspiring in a spontaneous epileptic fit, now seemed painfully never-ending - until at the first deep, stertorous inhalation, and first clonic shudders, the blood ran more freely in the bystanders' veins as well; and, lastly, to the immense relief of all concerned, was witnessed a characteristic, gradual awakening 'by steps'. The patient sat up of his own accord, looked about him calmly with a vague smile, as though asking what was expected of him. I asked him: 'What has been happening to you?' He answered, with no more gibberish: 'I don't know; perhaps I have been asleep.' That is how the first epileptic fit experimentally induced in man through the electric stimulus took place. So electroshock was born; for such was the name I forthwith gave it... Bini in 1942 suggested the repetition of ECT many times a day for certain patients, naming the method 'annihilation'. This results in severe amnesic reactions that appear to have a good influence in obsessive states, psychogenic depressions and even in some paranoid cases. 'Clustering' of treatments, shocking daily for three or four days followed by a three-day rest, is less intense but sometimes effectual. The method of annihilation has made possible studies of amnesia and of hallucinations, delirium, and moria occurring during the treatment, relating them to the personality factors in the patients (Bini and Bazzi, Polimanti). Flescher and Virgili have made systematic researches on amnesia and showed that spontaneous memory is more damaged than that of learned, didactic material and that automatic memory is still less disturbed. Depressed and aged patients show disturbances earlier than young or excited patients. The 'annihilation syndrome' has been compared by Cerquetelli and Catalano with the psychopathology following prefrontal leukotomy. They indicate close parallelism with the advantage of reversibility in the case of shock. These authors have also used shock successively to stop the symptoms of demerol mania quickly, following Mardnotti who used it with success in other forms of toxicomania. Broggi and others have also used ECT in progressive paralysis with at least temporary success. Ruggeri has used ECT in Parkinsonism and DeCrinis in disseminated sclerosis, observing attenuation of hypertonia. Electroshock has also been applied in certain general physical illnesses though all have a constitutional 'nervous' background. Recovery has been frequently reported in asthma, and Catalano and Cerquetelli, with Tomrnasi, have had success in psoriasis, prurigo, and alopecia areata. Mancioli, after having observed improvement in ozena in a schizophrenic patient treated with shock, found similar improvement after acroagonine injection and is pursuing the research with histological controls. Two other ideas both of which have perhaps as much relation to poetry as to science must be mentioned. The first is simply that the word 'shock' does not have the same meaning in neuropsychiatry as in general pathology. It is worth noting that any of our therapeutic methods such as prolonged sleep, narcoanalysis, insulin coma, epileptic corna, electronarcosis, etc., have in common the factor of the induction of a state of unconsciousness. The second idea has to do with the patient's fear of therapy, which leads some to want to stop it. On being asked the reason, they reply: 'I don't know, I am afraid.' 'Afraid of what?' 'I don't know, I have fear.' 'But were you worried, did you feel pain?' 'No, but I have fear.' There must be a vague recollection - organic memory - of the first 'terror-defence' reaction. I believe that name 'terror-defence' expresses the biological significance of epileptic fits. The terror phase, although taking place during unconsciousness, leaves specific bio-chemical and psychological changes in the organism that later emerge generically into the conscious sphere." (Old and New Information about Electroshock, Ugo Cerletti, American Journal of Psychiatry, 1950)
G. Shock Treatment, Brain Damage, and Memory Loss: A Neurological Perspective, John M. Friedberg
Shock Treatment, Brain Damage, and Memory Loss: A Neurological Perspective
John M. Friedberg, M.D.
American Journal of Psychiatry 134:9, September 1977. pp: 1010-1013.
The author reviews reports of neuropathology resulting from electroconvulsive therapy in experimental animals and humans. Although findings of petechial hemorrhage, gliosis, and neuronal loss were well established in the decade following the introduction of ECT, they have been generally ignored since then. ECT produces characteristic EEG changes and severe retrograde amnesia, as well as other more subtle effects on memory and learning. The author concludes that ECT results in brain disease and questions whether doctors should offer brain damage to their patients.
A 32 year old woman who had received 21 ECT treatments stated 5 years later.
"One of the results of the whole thing is that I have no memory of what happened in the year to year and a half prior to my shock treatments. The doctor assured me that it was going to come back and it never has. I don't remember a bloody thing. I couldn't even find my way around the town I lived in for three years. If I walked into a building I didn't even know where I was. I could barely find my way around my own house. I could sew and knit before. but afterward I could no more comprehend a pattern to sew than the man in the moon." (1. p. 22)
By 1928, 10 years before the introduction of electroconvulsive therapy, it was known that accidental death by cardiac arrest could result from as little as 70 to 80 milliamperes in the human (2). it was also known in this early period that voltage applied to the head, as in legal electrocution, produced hemorrhage and rupture of cranial contents. Ugo Cerletti (3) demonstrated that electricity in the range of 100 volts and 200 milliamperes is rarely fatal when the current path is confined to the head. but does evoke a grand mal seizure marked by a stereotyped succession of events. A tetanic muscular contraction, the "electric spasm,'' is followed after a latency of seconds by unconsciousness. a high voltage paroxysmal spike and sharp-wave discharge, and a clonic convulsion. Upon recovery of consciousness the subject is left with a transient acute brain syndrome. a high likelihood of permanent brain damage, and greater retrograde amnesia than is seen in any other form of head injury.
BRAIN DAMAGE IN EXPERIMENTAL ANIMALS
Before examining the premise that ECT damages human brains. a brief discussion of the lesions produced in animals by electrically induced convulsions is worthwhile. The many reports on this subject indicate that petechial hemorrhages scattered throughout both white and gray matter and concentrated in the path of the current are the most consistent finding. If animals are sacrificed after a delay of days or weeks following a convulsive series, hemosiderin pigment in phagocytes remains as evidence of vascular insult. Proliferation of glial cells. neuronal changes. and drop-out are also commonly reported.
In 1938, the year of the first use of ECT on a human being, Lucio Bini, Cerletti's collaborator. reported "widespread and severe ' brain damage in dogs with mouth to rectum electrode placement (4). At least seven subsequent animal studies employing conventional cranial electrodes supported his findings (5-11). These culminated in the exhaustive controlled experiment by Hans Hartelius in 1952 ( 12). This researcher found discernible vascular, glial. and neuronal changes in cats subjected to a maximum of 16 shocks. The animals were not paralyzed but were protected from physical injury during the seizure. Damage was slight but consistent. and the author concluded:
"The question of whether or not irreversible damage to the nerve cells may occur in association with ECT must therefore be answered in the affirmative.''
Furthermore, by examination of unlabeled slides alone Hartelius was able to correctly recognize 8 of 8 slides from shocked animals as well as 8 of 8 controls. Although he considered many of the vascular and glial changes to be reversible, there was no mistaking the brain of a shocked animal for that of a control.
Since that time, ECT in humans has been modified through the use of oxygen and muscle paralysis to reduce the incidence of bone fractures. Although it is believed that these modifications also reduce brain damage. there are no animal studies to support this idea. On the contrary recent work in England by Meldrum and associates (13. 14) on status epilepticus in pnmates suggests that the overexcited neuron by itself may be an important factor in seizure damage, especially in the hippocampus.
HUMAN BRAIN DAMAGE
Let us turn now to the neuropathological findings in humans who died during or shortly after ECT. As in lower animals. bleeding is the most frequent non- specific tissue response to injury and the one seen most often after electric shock. The first autopsy study in this country revealed brain damage identical to that seen in experimental animals. Alpers and Hughes (15) described the brains of 2 women who had received 62 and 6 shocks, respectively. The first woman's seizures had been suppressed by curare. Both brains showed hemorrhagic lesions around small blood vessels, rare- faction of tissue, and gliosis.
Throughout the 1940s similar reports continued to call attention to brain changes after ECT. including cases in which oxygen and curare had been administered (16). In 1948 Riese (17) added 2 more autopsy studies to the growing list and commented, "In all observations of sudden death after electric shock reported so far, petechial hemorrhages, cellular changes and some glial proliferation stand out prominently. as an almost constant whole."
Pathologists were especially interested in cases that discriminated between the direct effect of electricity and the mechanical and hypoxia effects secondary to convulsive motor activity. In 1953 Larsen reported on a 45-year old man who had been given 4 electroshocks in the course of 5 days. The ECT did not induce any convulsions. The subject died from pneumonia 36 hours after the fourth electroshock. At autopsy fresh subarachnoid hemorrhage was found in the upper part of the left motor region...."at the site where an electrode had been applied."(18)
In 1957 Impastato summarized 254 electroshock fatalities. Brain damage was the leading cause of death in persons under 40 years of age, and nearly one-fifth of all cerebral deaths were hemorrhagic (19).
Some physicians were alarmed by the evidence of human brain damage. In 1959 Allen reported 18 cases in which he had found signs and symptoms of neurological sequelae following ECT. He concluded, "It is probable that some damage, which may be reversible but is often irreversible, is inseparable from this form of treatment," and called for "more serious consideration of the entire procedure."(20)
In 1963, McKegney and associates (21) reported the case of a 23 year old man who became comatose 15 minutes after a single shock. The significance of this case was twofold: first, a complete physical and neurolgical examination was reportedly normal pnor to ECT, and seconded the ECT technique was contemporary and impeccable. The patient had received .6 mg of atropine, 16 mg of succinylcholine (Anectine), and forced oxygenation pre- and post-shock. ECT parameters were conventional. i.e.. 130 volts for .3 seconds. Four days later a brain biopsy showed diffuse degeneration of neurons with hyperplasia of astrocytes. The young man never regained consciousness and at autopsy 2 months later evidence of old hemorrhage was found in the brain. This was the last detailed report in the English-language literature.
The damaging effects of ECT on the brain are thoroughly documented. All told, there have been 21 reports of neuropathology in humans (22-36). it is interesting that, despite the importance of a negative finding there has not been a single detailed report of a normal human brain after shock.
ELECTROENCEPHALOGRAPHIC EFFECTS OF ECT
Like other insults to the brain, ECT produces EEG abnormalities. Diffuse slowing in the delta and theta range, increased voltage. and dysrhythmic activity are seen in all patients immediately following a series of bilateral ECT and, according to Blaurock and associates (37), may persist more than 6 months in 30 per cent of the cases. Such slowing suggests damage to the thalamus.
Sutherland and associates (38) showed that the side of the brain shocked with unilateral ECT could be predicted by double-blind assessment of EEG tracings.
The seizure thresholds of the hippocampus and other temporal lobe structures are the lowest in the brain; considerable interest has centered recently around "kindling'', or seizure induction by subthreshold stimulation of these areas in animals (39). The induction of a permanent epileptic disorder following ECT in humans was first reported in 1942 and other reports followed (40).
MEMORY LOSS
ECT is a common cause of severe retrograde amnesia, i.e.. destruction of memories of events prior to an injury. The potency of ECT as an amnestic exceeds that of severe closed head injury with coma. It is surpassed only by prolonged deficiency of thiamine pyrophosphate. bilateral temporal lobectomy, and the accelerated dementias, such as Alzheimer's.
After ECT it takes 5 to 10 minutes just to remember who you are. where you are. and what day it is. In the first weeks after a full course, retrograde and, to a lesser extent, anterograde amnesia are evident to the casual observer. But as time passes compensation occurs. As in other forms of brain injury. the subject is often oblivious to the residual deficit. Unless specific memories essential to daily living are discovered to be unavailable the victim may never know for sure the extent of memory loss.Unless sensitive tests for spontaneous recall of personal preshock data are employed no one else will know either.
The memory loss following ECT generally follows Ribot's law for all pathological amnesias: the new dies before the old. This, of course, is the opposite of normal forgetting. Squire, however, has shown that the loss may extend to items learned more than 30 years before (41).
The effect of ECT on memory was common knowledge within a few years of its introduction. There were reports of persons who forgot they had children (42. 43), although most amnesias involved humbler matters. such as the woman who forgot how to cook familiar dishes (44) and another who couldn't remember her own clothing and demanded to know who had put the unfamiliar dresses in her closet (45). Some doctors dismissed these sequelae as trivial or transient, although one psychiatrist remarked that psychotherapy was useless in patients undergoing ECT because they couldn't remember "'either the analyst or the content of the analytic sessions from one day to the next.'' (46).
Numerous such case reports finally led to a definitive study of the effects of ECT on memory by Irving Janis in 1950 (47). He found that all 19 subjects in a controlled prospective investigation had significant memory loss 4 weeks after ECT, compared to negligible losses among control subjects. He also noted that these losses may involve events of early childhood dating back 20 to 40 years, with the more recently en- coded memories being the most vulnerable. Patient E. for example. a 38-year-old woman, had told Janis in an interview prior to ECT that thyroid medication had caused heart palpitations and panic which led to her admission to the psychiatric hospital. When asked after a course of 10 shocks if she had ever taken thyroid she responded: "I don't think so."
In the late 1940s. when the enthusiasm for ECT seemed to have passed its peak (48). Lancaster and associates (49) advocated the use of unilateral non-dominant ECT in treating patients who earn their livelihood with retained knowledge. In this variant the current path and most of the damage is confined to the nonverbal side of the brain, usually the right hemisphere. This exploits the well-known neurological phenomenon of anosognosia. or denial. that is associated with right-hemisphere lesions - victims can't verbalize their difficulties. They complain less. Cohen and associates (50). however. using design-completion tests. proved that shock to the right hemisphere produces its own kind of memory loss: visual and spatial. Inglis found in 1970 (51) that the effects of unilateral ECT were comparable to those of right and left temporal lobectomy, with identical impairment of memory and learning.
Recently there has been a good deal of human experimentation in a futile effort to find electrode placements that eliminate amnesia. As the use of ECT has shifted from state hospitals to private practice, the literature has focused more and more on memory loss.
Although some studies have purported to show provement of learning ability after ECT, not one u sham ECT as a control and few used any controls at all.(1)
In regard to more general intellectual ability, a study in 1973 (54) showed that the performance on the Bender Gestalt perceptual motor test of 20 institutionalized subjects who had received 50 or more ECT treatments 10 to 15 years before testing was significantly impaired compared to the performance of 20 carefully matched control subjects who had not received ECT. The authors inferred that ECT had caused permanent be damage.
MECHANISM OF ACTION OF ECT
The mechanism of action of ECT can now be summarized on the basis of evidence accumulated since introduction. Penfield and Perot showed in the 1950's that memory traces may be evoked by direct electrical stimulation of the temporal lobe cortex. and nowhere else (55). Scoville and Milner (56) discovered that bilateral hippocampal resection utterly abolished ability to remember any new material. resulting in a catastrophic inability to learn. From numerous studies of the neuropathology of the amnestic-confabulatory syndrome of Korsakoff it is known that the mammillary bodies. the dorsal median nuclei of the thalamus and the gray matter surrounding the third ventricle a aqueduct are essential to the general memory process. All of these critical brain structures are just beneath the thin squamous plate of the temporal bone. with seven centimeters of the electrodes. in the direct path and highest density of the current during ECT.
CONCLUSIONS
From a neurological point of view ECT is a method of producing amnesia by selectively damaging the temporal lobes and the structures within them. When it was first introduced it was only one of several methods of producing brain damage employed in psychiatry, including insulin coma (1927)* camphor and Pentylenetetrazol (Metrazol) injections (1933). and prefrontal lobotomy (1935), it is the only such method from that era still used on a large scale. It is highly unlikely that ECT, if critically examined, would be found acceptable by today's standards of safety.
From a neurological point of view ECT produces form of brain disease. with an estimated incidence new cases in the range of 100.000 per year (57). Many psychiatrists are unaware that ECT causes brain damage and memory loss because numerous authorities and a leading psychiatric textbook (58) deny these facts.
Others, who know of its effects argue that the interruption of unpleasant states of mind is worth the damage. Some are beginning to give the client a truly informed choice, although state laws still allow ECT to be imposed if the doctor feels that ''good cause'' exists.
Assuming free and fully informed Consent, it is well to reaffirm the individual's right to pursue happiness through brain damage if he or she so chooses. But we might ask ourselves whether we, as doctors sworn to the Hippocratic Oath, should be offering it.
REFERENCES
1. Friedberg J: Shock Treatment is Not Good For Your Brain. San Francisco. Glide Publications. 1976
2. Jaffe R: Electropatholohy: a review of the pathologic changes produced by electric current. Arch Neurol Psychiatry 5:838- 864. 1928 3. Cerletti U: Electroshock therapy. in The Great Physiodynamic Therapies in Psychiatry. Edited by Sackler A. Sackler R. Sackler M. et al. New York. Hoeber-Harper. t956, pp 91-120 4. Bini L: Experimental researches on epileptic attacks induced by the electric current. Am J Psychiatry 94:172-174. 1938 5. Heilbrunn G. Lieben E: Biopsies on the brain following artificially produced convulsions. Arch Neuroi Psychiatry 46:548-552, 1941 6. Neubuerger KT. Whitehead RW. Rutledge RK. et al: Pathologic changes in the brains of dogs oven repeated electric shocks. Am J Med Sci 204:381-387. 1942 7. Heilbrunn G. Weil A: Pathologic changes in the central nervous system in experimental electric shock. Arch Neurol Psychiatry 47:918, 1942 8. Alpers 8J. Hughes J: Changes in the brain after electrically in- duced convulsions in cats. Arch Neurol Psychiatry 47:385. 1942 9. Alexander L, Lowenbach H: Experimental studies on electroshock treatment: the intracerebral vascular reaction as an indicator of the path of the current and the threshold of early changes within the brain tissue. J Neuropathot Exp Neurol 3:139, 1944 10. Ferraro A. Roizin L. Helfand M: Morphologic changes in the brain of monkeys following convulsions electrically induced. J Neuropathol Exp Neurol 5:285. 1946 11. Ferraro A. Roizin L: Cerebral morphologic changes in monkeys subjected to a large number of electrically induced convulsions (32-100). Am J Psychiatry 06:278. 1949 12. Hanelius H: Cerebral changes following electrically induced convulsions. Acta Psychiat et Neurol Scand Supplement 77. I 952 13. Meldrum B. Roger V, 8riericy J: Systemic factors and epileptic brain damage. Arch Neurol 29:82-87. 1973 14. Meldrum B. Honon R. 8rierley J: Epileptic brain damage in adolescent baboons following seizures induced by allylglycine. Brain 97:407-418. 1974 15. Alpers BJ. Hughes J: The brain changes in electrically induced convulsions in the human. J Neuropathol Exp Neurol 1:173. 1942 16. Ebaugh FG. Barnacle CH. Neubuerger KT: Fatalities following electric convulsive therapy: report of two cases. with autopsy. Arch Neurol Psychiatry 49:107. 1943 17. Riese W: Report of two new cases of sudden death after electric shock treatment with histopathological findings in the central nervous system. J Neuropathol Exp Neurol 7:98-100. 1948 18. Larsen EG. Vna-Jansen G: Ischaemic changes in the brain following electroshock therapy. Acta Psychiat et Neurol Scand 28:75-80. 1953 19. Impastato D: Prevention of fatalities in electroshock therapy. Dis Nerv Syst 18:34-75, 1957. (author's comment: Impastato, himself a shock doctor, estimated a DEATH RATE of 1/200 in this paper. Dr. Max Fink has recently alchemized this figure into 1/200 memory loss but the state of Texas reported a 1/200 death rate in 1994.) 20. Allen 1: Cerebral lesions from electric shock treatment. NZ Med J 58:369. 1959 21. MclCegney FP. Panzetta AF: An unusual fatal outcome of electro-convulsive therapy. Am 1 Psychiatry 120:398-400. 1963 22. Ebaugh FG. Barnacle CH. Neubuerger KT: Fatalities following electric convulsive therapy. A report of 2 cases with autopsy findings. Trans Am Neurol Assoc. June 1942. p 36 23. Gralnick A: Fatalities associated with electric shock treatment of psychoses: report of two cases with autopsy observations in one of them. Arch Neurol Psychiatry 51:397. 1944 24 Jetter WW: Fatal circulatory failure caused by electric shock therapy. Arch Neurol Psychiatry 51:57. 1944 25. Meyer A. Teare D: Cerebral fat embolism after electrical con- vulsion therapy. Br Med J 2:42. 1945 26. Sprague DW. Taylor RC: The complications of electric shock therapy with a case study. Ohio State Med J 44:51-54. 1948 27.Will OA Jr. Rehfeidt FC: A fatality in electroshock therapy: report of a case and review of certain previously described cases. J Nerv Ment Dis 107:105-126. 1948 28.Martin PA: Convulsive therapies: review of 511 cases at Pontiac State Hospital. J Nerv Ment Dis 109:142-157. 1949 29. Riese W. Fultz GS: Electric shock treatment succeeded by complete flaccid paralysis. hallucinations. and sudden death: case report with anatomical findings in the central nervous system Am J Psychiatry 106:206-211. 1949 30. Liban E. Halpern L. Rozanski J: Vascular changes in the brain in a fatality following electroshock. J Neuropathol Exp Neurol 10:30W318. 1951 31. Corsellis J. Meyer A: Histological changes in the brain after uncomplicated electro-convulsive treatment. J Ment Sci 100.375- 383. 1954 32. Madow L: Brain changes in electroshock therapy. Am I Psychiatry 113:337-347. 1956 33. Faurbye A: Death under electroshock treatment. Acta Psychiatrica et Neurologica 17:39.1942 34. Maclay WS: Death due to treatment. Proc Soc Med 46:13-20 1953 35. Matthew JR. Constan E: Complications following ECT over a three-year period in a state institution. Am J Psychiatry 120:1 1 19-1 120. 1964 36. Barker J. Baker A: Deaths associated with electroplexy. J Ment Sci 105:339-34S 1959 37. Blaurock M. Lorimer F. Segal M. et al.: Focal electroencephalographic changes in unilateral electric convulsion therapy. Arch Neurol Psychiatry 64:220-226. 1950 38. Sutherland E. Oliver J. Knighl D: EEG. memory and confusion in dominant. non-dominant and bi-temporal ECT. Br J Psychiatry:1059-1064. 1969 39. Wada J. Osawa T: Spontaneous recurrent seizure state induced by daily electric amygdaloid stimulation in senegalese baboons (papio papioh Neurology 26:273-286. 1976 40. Parfitt D: Persisting epilepsy following shock therapy. Br Med 2:514. 1942 41. Squire L: A thirty-year retrograde amnesia following electroconvulsive therapy in depressed patients. Presented at the 3rd annual meeting of the Society for Neuroscience. San Diego.1973 42. Tyler B. Lowenbach H: Polydiurnal electric shock treatment in mental disorders. NC Med J 8:577-582. 1947 43. Medlicott R: Convulsive therapy. Results and complications in four hundred cases. NZ Med J 47:338. 1948 44. Brody M: Prolonged memory defects following electrotherapy. J Ment Sci 90 779. 1944 45. Zubin J: Objective studies of disordered persons. in Methods of Psychology. Edited by Andrews T. New York. John Wiley and Sons. 1948. pp 595-623 46. Stainbrook E: Shock therapy: psychologic theory and research. Psychol Bull 43:21-60. 1956 47. Janis 1: Psychologic effects of electric convulsive treatments. Part 1: post-treatment amnesias. J Nerv Ment Dis 3:359-382. 1950 48. Spiegel E (ed): Progress in Neurology and Psychiatry: An Annual Review. New York. Grune h Stratton. 1957 49. Lancaster N. Steinen R. Frost 1: Unilateral electro-convulsive therapy. J Ment Sci 104:221-227. 1958 *Sham ECT, an essential control technique has been employed in only two studies which were tests of efficacy, not tests of memory. Neither study showed any superiority of ECT over controls. Revised version of a paper presented at the 129th annual meeting of the American Psychiatric Association, Miami Beach. Fla. May 1W 14. 1976. |
Conclusion:
- Historically psychiatry has a long history of hurting, torturing and injuring people.
- We predict that ECT will soon be outlawed by 2015 because of lawsuits currently in the trial stages.
- A single ECT treatment passes enough electricity through your brain to light an 84 watt light bulb for 6 seconds or a 500 watt halogen light for 1 second. And we call this medicine? Chemical psychiatrists are on record for saying that if the same current was passed through the heart, it would surely kill you. But, they argue, passing it through the brain does not kill you! Sure! You can also cut off your arms, legs, ears and tongue and you will still live!
- Since DC current delivers 27% more power than AC current, the actual corresponding wattage into household current would be 107 Watt light bulb for six seconds or 635 watt halogen light for 1 second.
- "When a patient is drugged or shocked by a psychiatrist, it usually says more about the doctor's spiritual failure than about the "diagnosis" of the patient" (The Heart of Being Helpful, Peter Breggin, 1997 AD. p 81)
- Leave it to chemical psychiatrists to think shocking the brain would cure anger, rage, depression or anxiety.
By Steve Rudd: Contact the author for comments, input or corrections.
Send us your story about your experience with modern Psychiatry
HOW i got a cure for stroke
ReplyDeleteI really want to take this time out to show my appreciation to a doctor who advised me correctly. I had stroke for 12 years and my full left side was paralyzed because of this i could say i was half human because i could not function where others are functioning. I knew i needed help and i began to search and i saw his contact from a testimony some people were giving, i never believed because i have tried so many medicines and therapies yet no cure. I still contacted him to see what he had to offer. I got the medicine (herbal medication) he told me about and i could not believe my eyes. In a matter of 3 months i was completely okay. If you have any stroke related illness or paralysis feel free to reach him for info and cure on (josephalberteo@gmail.com) he treated me and he can treat you too. cheers.